

Adolescent Idiopathic Scoliosis: Is Your Approach Effective?
By: Cheryl Canon, PT, DPT; OptimisPT Director of Implementation and Compliance
Nothing drives you more to learn about a specific topic as when your own child is affected by it. Three months ago my ten year old daughter had her yearly checkup, and her primary doctor did an Adam’s Test. The Adam’s Forward Bend Test is used to detect structural or functional scoliosis. When I saw it was positive, I was very surprised. I’ve screened my daughter in the past year and the amount of rib hump I observed was far beyond what I ever thought could be possible in such a short period of time. How was it possible that I didn’t notice what I was seeing in front of me?
Adolescent Idiopathic Scoliosis (AIS) is the most common form of scoliosis and, by definition, occurs in children aged 10 through skeletal maturity and is found in as many as 4 in 100 adolescents. AIS is a progressive condition, so the key is to try and catch the condition early on before the spinal curvature gets larger and more difficult to treat. A straight spine has a curve of 0º, any curve greater than 10º is considered scoliosis.
My first thought was, “If it has developed this quickly from the last time I assessed my daughter, how fast is this going to progress?”
A combination of following individual factors is used to predict curve progression:
- age at presentation/Risser score (future growth potential),
- gender (prevalence higher in females for progression. Also includes when a menstrual cycle started), and
- the magnitude of the curve at presentation (Cobb angle).
If a rib hump is seen during an Adam’s forward bend test, a scoliometer can be used to determine if a patient should have a radiograph.
Adam’s Test

Scoliometer
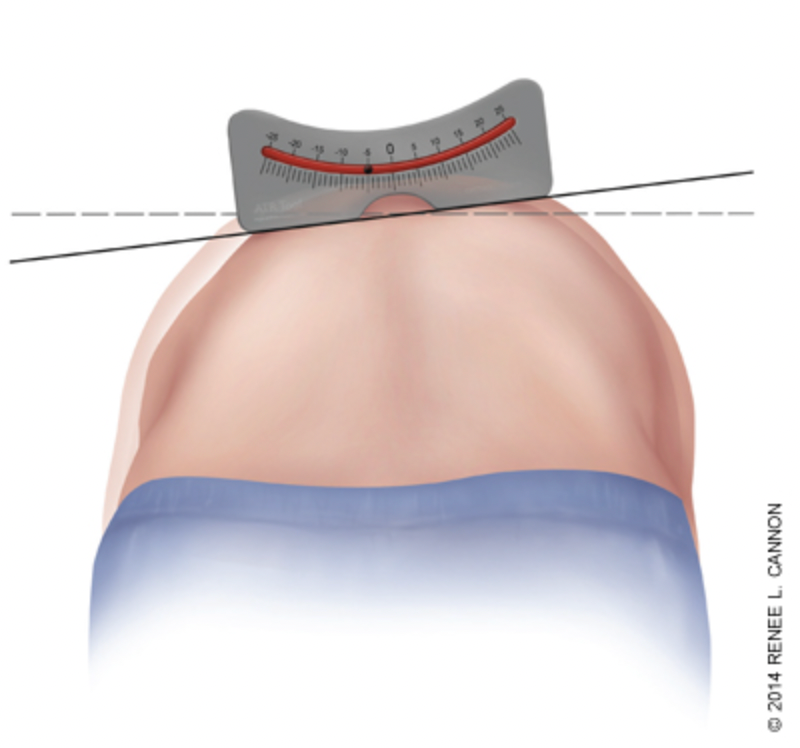
Generally, if using the scoliometer you see trunk rotation less than 5 degrees it is insignificant and may not require follow-up. A measurement of 5 to 9 degrees at least warrants reexamination in six months and a measurement of 10 degrees or greater requires an X-Ray for Cobb angle measurement and a Risser score. My daughter had a 12 degree measurement with the scoliometer during the Adam’s Test. She was referred for plain films.
This was my daughter’s plain films:
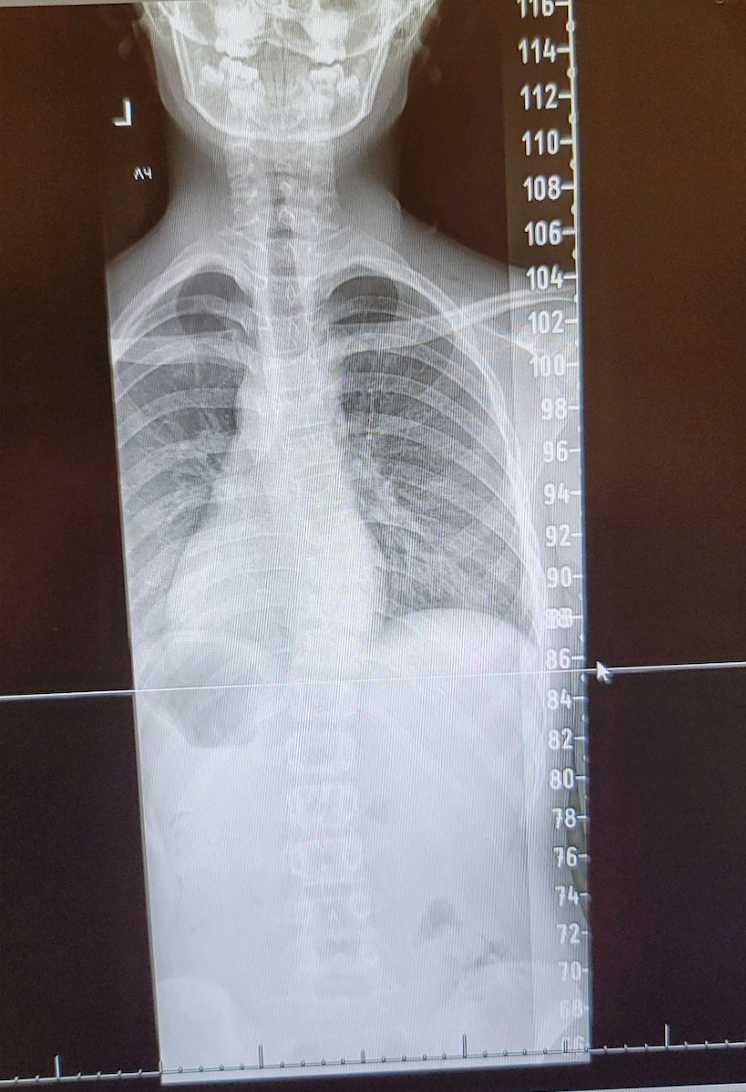
Her Cobb angle measured 26 degrees and an X-Ray of her hand was taken to determine her Risser sign, which was Risser 2. The Cobb angle is defined as the greatest angle at a particular region of the vertebral column, when measured from the superior endplate of a superior vertebra to the inferior endplate of an inferior vertebra. The angle formed at the intersection of these two lines is the Cobb angle.
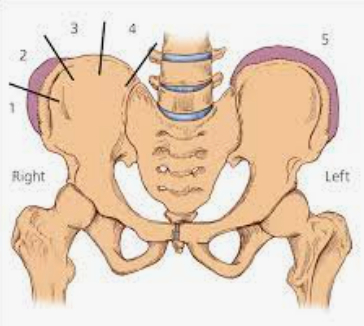
Much of the time the Risser classification can be taken from the iliac crest. The Risser classification is used to grade skeletal maturity based on the level of ossification and fusion of the iliac crest apophysis, basically how much growth is still anticipated. A Risser 2 is illustrated below on the right iliac crest in comparison to what a Risser 5 would look like on the left iliac crest. A patient with stage 0 will still have open growth plates in most of the long bones and will likely be younger than age 16 (female) or 18 (male). A patient with stage 5 will have no open growth plates in the long bones. Age, along with the Cobb angle and the Risser sign helps in determining how aggressive treatment may need to be.
I didn’t know any of this basic information prior to my daughter’s X-Ray, and I consider myself a pretty decent therapist. I’ve been through an orthopedic residency, passed my OCS exam, and obtained good outcomes with patients. I felt I’d be able to do a decent job helping my daughter, but since this was my daughter, I wanted to help ensure I was as knowledgeable about AIS as I could be. So I took some continuing education classes prior to my daughter’s X-Ray. Four of them, to be exact (thank goodness for on-demand courses by exceptional therapists). What I also learned, however, is that I really didn’t know what I didn’t know. If I had applied what I “thought” would have been a good approach to intervention, I would have likely made my daughter’s curve worse rather than better. I would have attempted to strengthen the muscles I thought were “stretched” on the convex side of the curve, stretched the muscles I thought were shortened on the concave side of the curve, then done a lot of shoulder girdle and core strengthening exercises. Sidebending exercises, stretching…all seemed like a good plan of care. I would have been ½ wrong. While these activities can improve body function and performance, they have no effect on the prevention or control of scoliosis.
I learned through the four continuing education courses that scoliosis specific exercises are essential for helping to prevent curve progression, and they are very different from our traditional exercises, based on each specific patient’s curve pattern. Asymmetries occur in 3 dimensions: 1) Front to back, 2) Side to side, 3) Rotation. Someone with a lumbar curve will need completely different scoliosis exercises from someone with a thoracic or thoracolumbar curve.
After my daughter’s X-Ray she was referred to ortho. Knowing the recommendations from the International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) helped to make the decision on how aggressively to treat my daughter to prevent further progression of the curve.
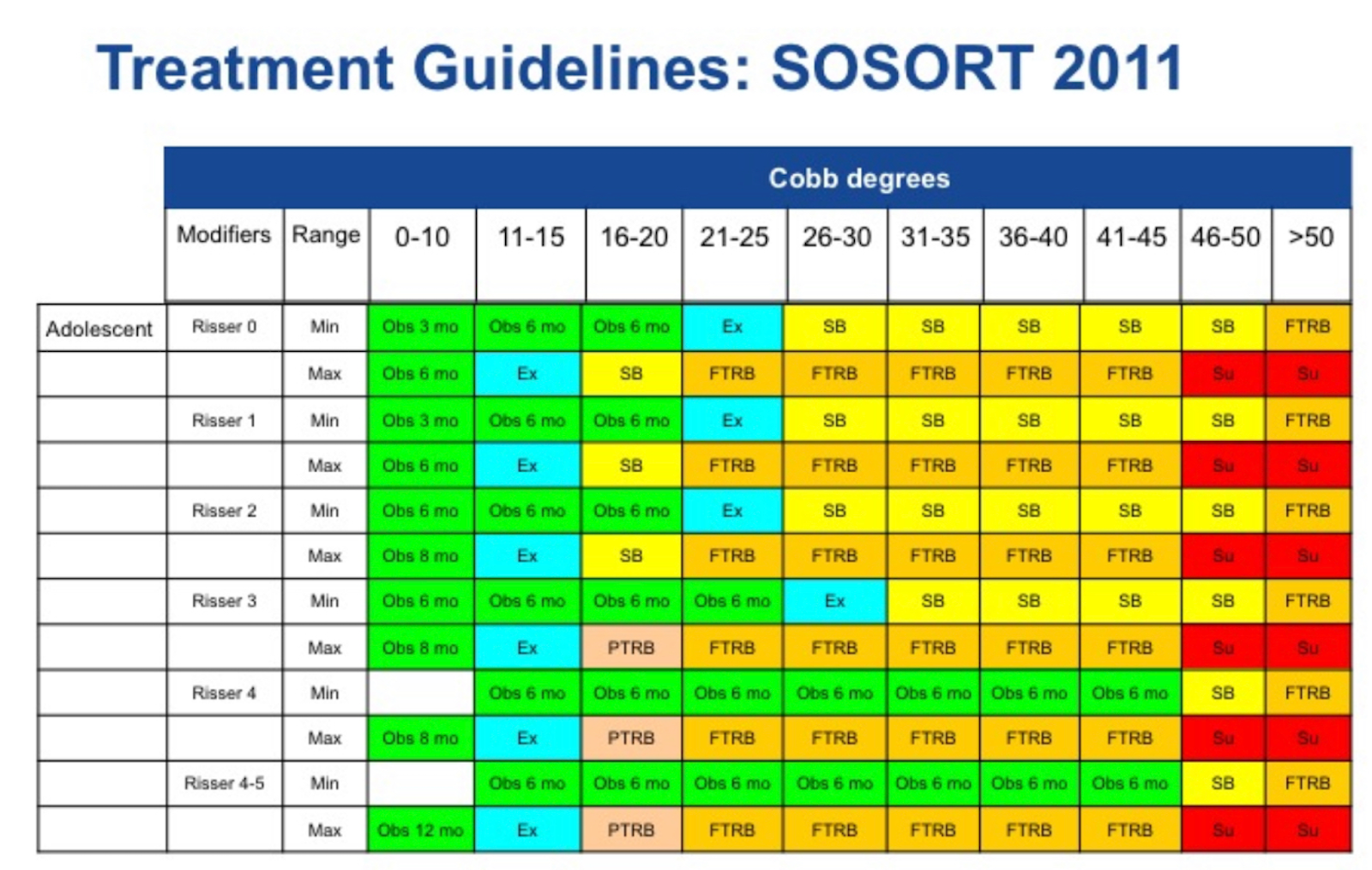
With a Cobb of 26 degrees and a Risser 2, soft-bracing at a minimum to full-time rigid brace and Physiotherapeutic scoliosis-specific exercises (PSSE) is recommended. When she saw the orthopedic specialist, he indicated that he calculated a Cobb of 23 degrees, which puts her in the middle of soft bracing to rigid bracing. My ten year old daughter would have to wear the rigid brace at least 16 hours a day for it to be effective. There are great publications on the effectiveness of bracing and PSSE at the end of this blog.
I learned a lot through this experience, and I feel I have so much more to learn. The literature and guidelines provide a great reference to help therapists, patients and families of patients decide how aggressively to treat in order to avoid surgery and prevent curve progression. The challenge is not knowing if and by how much a curve will progress without intervention. I learned that even a highly specialized therapist may not be the most effective in preventing progression of the curve if they have not had training in PSSE. I learned, as a therapist, goal setting for AIS can be challenging to ensure continued reimbursement over the years that you may be treating a patient that has a lot of growth left. I learned the importance of working with the entire rehab team of the orthopedic surgeon, orthotist and family for education and being well-informed to decide the best path for the patient, and that a patient-centered approach for AIS, as with all patients, is essential. I learned that bracing along with PSSE can not only have the potential to prevent curve progression, but in some cases, can even decrease the COBB angle; a good goal is 50% decrease in Cobb angle.
We are in a great position, as therapists, to help detect scoliosis in our communities. Volunteering at a local school to screen students, offering free scoliosis screenings in our clinics, and creating a network of specialists to refer to if we’re not specialized in PSSE can be a great way to help detect what may otherwise go unnoticed in many adolescent individuals. An Adam’s forward bend test, combined with a scoliometer, is a safe, noninvasive, and informative means of determining if there is further cause for concern. I just purchased a scoliometer so that I can monitor any changes in my daughter, and we’re still in the process of setting up an evaluation with an orthotist. I will be setting up an evaluation with a physical therapist that specializes in PSSE, so that I can learn the very best exercises and postural activities to provide the best outcomes possible for my daughter. I had to learn that sometimes, reaching out to someone that is more highly trained in an area, is the best course of action.
REFERENCES
2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O’Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi: 10.1186/s13013-017-0145-8. eCollection 2018. Review. PMID: 2943549
Adolescent Idiopathic Scoliosis Part 1: Definition & Diagnosis, Part 2: Clinical and Radiological Evaluation, Part 3: Indications, Guidelines & Goals of Treatment, and Part 4: Specific Exercises to the Condition, presented by Cindy Marti
Guidelines on “Standards of management of idiopathic scoliosis with corrective braces in everyday clinics and in clinical research”: SOSORT Consensus 2008. Negrini S, Grivas TB, Kotwicki T, Rigo M, Zaina F; international Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Scoliosis. 2009 Jan 16;4:2. doi: 10.1186/1748-7161-4-2. PMID: 19149877
https://advance-physicaltherapy.com/2017/scoliosis-specific-exercises/
Fan, Y., Ren, Q., To, M.K.T. et al. Effectiveness of scoliosis-specific exercises for alleviating adolescent idiopathic scoliosis: a systematic review. BMC Musculoskelet Disord 21, 495 (2020). https://doi.org/10.1186/s12891-020-03517-6
Yagci G, Yakut Y. Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment. Prosthet Orthot Int. 2019 Jun;43(3):301-308. doi: 10.1177/0309364618820144. Epub 2019 Jan 10. PMID: 30628526.


